A lecture about life challenges after laryngectomy including lymphedema care can be viewed on YouTube.
Lymphedema
The lymph vessels drain fluid from tissues throughout the body and allow immune cells to travel throughout the body. Lymphedema is a localized lymphatic fluid retention and tissue swelling caused by a compromised lymphatic system. It can be caused by surgery, radiation, and by the cancer.
Lymphedema, a common complication of radiation and surgery for head and neck cancer, is characterized by an abnormal accumulation of protein-rich fluid in the space between cells which causes chronic inflammation and reactive fibrosis of the affected tissues. Lymphedema generally starts eight to twelve weeks after initiation of radiation therapy and can be a life long issue.
Radiation creates scarring which interferes with the function of the lymphatics. The cervical lymph nodes are generally removed when the cancer is excised. When the surgeons remove these glands they also take away the drainage system for the lymphatics and cut some of the sensory nerves. Unfortunately, most of the severed lymphatics and nerves are permanently cut. Consequently, it takes longer to drain the area, resulting in swelling. Like flooding after a heavy rain when the drainage system is broken, the surgery creates a backup of lymphatic fluid that cannot drain adequately, as well as numbness of the areas supplied by the severed nerves (usually in the neck, chin, and behind the ears). As a result, some of the lymphatic fluid cannot re-enter the systemic circulation and accumulates in the tissues.

There are two types of lymphedema that can develop in patients with head and neck cancer: an external visible swelling of the skin or soft tissue and an internal swelling of the mucosa of the pharynx and larynx which can also interfere with swallowing. Lymphedema generally starts slowly and is progressive, rarely painful, causes discomfort in the form of a sensation of heaviness and achiness, and may lead to skin changes.
Lymphedema
The lymph vessels drain fluid from tissues throughout the body and allow immune cells to travel throughout the body. Lymphedema is a localized lymphatic fluid retention and tissue swelling caused by a compromised lymphatic system. It can be caused by surgery, radiation, and by the cancer.
Lymphedema, a common complication of radiation and surgery for head and neck cancer, is characterized by an abnormal accumulation of protein-rich fluid in the space between cells which causes chronic inflammation and reactive fibrosis of the affected tissues. Lymphedema generally starts eight to twelve weeks after initiation of radiation therapy and can be a life long issue.
Radiation creates scarring which interferes with the function of the lymphatics. The cervical lymph nodes are generally removed when the cancer is excised. When the surgeons remove these glands they also take away the drainage system for the lymphatics and cut some of the sensory nerves. Unfortunately, most of the severed lymphatics and nerves are permanently cut. Consequently, it takes longer to drain the area, resulting in swelling. Like flooding after a heavy rain when the drainage system is broken, the surgery creates a backup of lymphatic fluid that cannot drain adequately, as well as numbness of the areas supplied by the severed nerves (usually in the neck, chin, and behind the ears). As a result, some of the lymphatic fluid cannot re-enter the systemic circulation and accumulates in the tissues.
Humid weather and high altitude can aggravate lymphedema. High humidity makes
it difficult to perspire and more fluid may accumulates within the body which
can increase lymphedema. Also because barometric pressure is reduced at high
altitudes, this can lead to the exacerbation of the
condition.
The lymphatic system is similar to the gutter in draining
There are two types of lymphedema that can develop in patients with head and neck cancer: an external visible swelling of the skin or soft tissue and an internal swelling of the mucosa of the pharynx and larynx which can also interfere with swallowing. Lymphedema generally starts slowly and is progressive, rarely painful, causes discomfort in the form of a sensation of heaviness and achiness, and may lead to skin changes.
Lymphedema
has several stages:
· Stage 0: No
swelling, but a sense of heaviness in the neck
·
Stage 1a: Visible mild swelling without pitting. Reversible
·
Stage 1b: Visible mild swelling with pitting. Reversible
·
Stage 2: Firm
pitting swelling that is irreversible. No visible tissue changes
· Stage
3: Irreversible tissue changes with scarring
and fibrosis
Lymphedema
of the head and neck can cause several functional impairments.
These include:
- Difficulty in breathing
- Impairment
in vision
- Motor
limitations (reduced neck motion, jaw tightness or trismus, and chest
tightness)
- Sensory
limitations
- Speech, voice and swallowing problems (inability
to use an electrolarynx, difficulty in articulation, drooling, and loss of
food from mouth)
- Feeling congested
- Ear pain
- Emotional issues (depression, frustration, and embarrassment)

Lymphedema of the chin and neck
Over time, the
lymphatics find newer way of drainage, and the swelling and neck tightness generally
goes down. Sleeping with the upper body in an elevated position can use gravity
to speed the process of lymph fluid drainage.
Treatment of lymphedema includes:
- Manual lymph drainage ( face and neck, deep
lymphatics, trunk, intra oral)
- Compression bandages and garments
- Use of a tactile lymphatic pump
- Remedial exercises
- Skin care
- Elastic therapeutic tape (Kinesiotape)
- Oncology rehabilitation
Definite diagnosis of lymphedema can be made by lymphoscintigraphy
and MRI. Diuretics, surgical removal (debulking), liposuction, compression
pumps, and elevation of the head alone are ineffective treatments.
A lymphedema treatment specialist can perform and teach manual lymph drainage that can help in reducing edema. Manual
lymphatic drainage is a massage-like technique that is performed by
specially trained physical therapists. It evolves gentle skin massage to drain edema fluid from the body's periphery into the blood stream towards the heart in an effort to enhance
filling of the cutaneous lymph vessels, dilation and contractility of the lymphatic vessels, and recruit unused pathways for lymph flow..Movement and exercise are also important in aiding lymphatic drainage.

Manual massage to reduce lymphedema

A head and neck lymphedema therapist can select non-elastic bandages or compression garments that are worn at home. These place gentle pressure on the affected areas to help move the lymph fluid and prevent it from refilling and swelling. Application of bandages should be done as directed by a specialist. There are several options, depending on the location of the lymphedema to improve comfort and avoid complications from pressure on the neck.

Bandages used to reduce lymphedema


Compression garment used to reduce lymphedema
There are also specific exercises that can reduce the neck tightness and increase the range of neck motion. One needs to perform these exercises throughout life to maintain good neck mobility. This is especially true if the stiffness is due to radiation. Receiving treatment by experienced physical therapies who can also break down the fibrosis is very helpful. The earlier the intervention the better.
A new treatment modality that reduces lymphedema,
fibrosis, and neck muscle stiffness using external laser is also available. This method uses a low energy laser beam administered by
an experienced physical therapist. The laser beam penetrates into the tissues where it is absorbed by cells and changes their metabolic processes. The beam is generated by the LTU-904 Portable Laser Therapeutic Unit. This treatment can
reduce the lymphedema in the neck and face and increase the head’s range of
motion. It is a painless method that is done by placing the laser instrument
at several locations over the neck for about 10 seconds’ intervals.

Hand held laser for lymphedema treatment

There are physical therapy experts in most communities who specialize in treating lymphedema, and reducing swelling and edema. It is advisable that one consults their surgeon if physical therapy is a
good therapeutic option for their lymphedema.
The National Lymphedema Network has a web site that can assist in locating a lymphedema specialists in North America, Europe and Australia.
The Lymphedema Association of North America has a website that can assist in locating a lymphedema specalist in North America.
A facial and neck self massage guide is also available.
The National Lymphedema Network has a web site that can assist in locating a lymphedema specialists in North America, Europe and Australia.
The Lymphedema Association of North America has a website that can assist in locating a lymphedema specalist in North America.
A facial and neck self massage guide is also available.

The lymphatic system in the neck
A slide presentation about the diagnosis and treatment of lymphedema in head and neck cancer patients is available. It was presented at the
Milton J. Dance, Jr. Head and Neck Center 15th
Annual Conference on Head &Neck Rehabilitation on October 26, 2012.




A presentation by Jan Lewin, Ph.D. from MD Anderson about their program treating lymphedema
Skin numbness after surgery
The cervical lymph nodes, or
glands, are generally surgically removed when the cancer is excised. When the
surgeons remove these glands, they also cut some of the sensory nerves that
supply the lower facial and neck skin. This creates numbness in the areas
supplied by the severed nerves. Some of the numb areas may regain sensation in
the months following the surgery, but other areas may remain permanently numb.
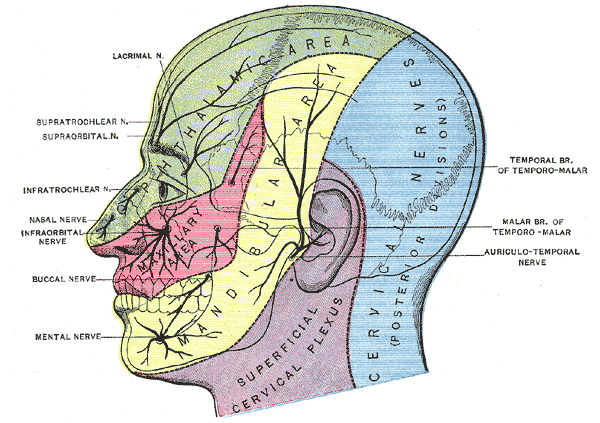
Skin nerves of the face and neck
Most individuals become accustomed
to the numbness and are able to prevent damage to the skin from sharp objects,
heat or frost. Men learn not to injure the affected area when shaving by using
an electric shaver.
The numb skin should be protected
from sun burn by applying sunscreen and/or by shielding it with a garment.
Frostbite can be prevented by covering the area with a scarf.

Neck and shoulder pain after surgery and radiation
Persistent difficulty with movements of the shoulder, neck,
face, and jaw often result from head and neck surgery. These difficulties are
the result of the removal or manipulation of the region’s muscles, nerves, and
lymphatic and blood vessels during surgery and their exposure to radiation
therapy. Often, varying degrees of muscle weakness, scar tissue, and lymphedema
are lifelong complications that can affect a person’s neck and shoulder health.
Because of the proximity of the lymphatic vessels to nerves that
innervate the face, neck, and shoulder, they are frequently removed or damaged
during surgery of the head and neck. Excision of the cancer may require
manipulation or removal of the facial or spinal accessory nerves. The removal
of the nerves effects of the movement of face, neck, and shoulder complex
muscles. The effect is generally temporary after nerve manipulation during
surgery, but may be permanent if the nerve has been severed. Nevertheless,
regeneration of the nerves may occur within six weeks to several years.
Following complete severance of the nerves that innervate neck
and shoulder muscles, they become limp and fail to stabilize the scapular
joints (between the scapula and thorax and the humeral bone)(see Figure below). The
affected joints are, therefore, at risk for further injury.

The shoulder complex
When the scapular
stabilizer muscles (middle trapezius and rhomboids) are compromised, (see Figure below) it is
difficult to maintain an erect posture that allows for proper shoulder
retraction. Without adequate retraction of the shoulder girdle, the
glenohumeral joint (between the scapula and the humeral bone) cannot elevate
the arm through a full range of 180 degrees. Lifting the arm when the scapula
is in a protracted (forward) position creates a bony block from the humeral
bone hitting the shoulder blade (acromion process) and does not allow full
motion.

Scapular muscles
Partial dislocation of the shoulder joint (glenohumeral subluxation) can take place because of the lack of muscle stabilization in the
shoulder. This creates shoulder instability and an inability to lift the arm
through the full range of motion at the shoulder. Further damage to the
shoulder joint and rotator cuff can occur with repetitive attempts to use the
arm when it is weak.
Reduced stability of the joints also creates a structural strain
on the neurovascular bundle of the shoulder and surrounding muscles, producing myofascialpain syndrome (chronic dull radiating pain from neck to hand) through the
neck, shoulder, and arm.
The “leaning forward” posture that gradually develops lengthens
the upper back muscles and fascia and shortens the muscles in the chest and
neck region. This out of balance posture generates increased strain on the
upper back, neck, and shoulder joints.
Radiation therapy further aggravates the situation because of
the formation of scar tissue on top of existing scars from the surgical process
and complicates one’s ability to stretch tight areas. Tissues contractions can
also develop in the chest and neck.
Scar formation through fibrin formation constitutes the body’s
healing mechanism following injury and trauma, such as surgery or radiation.
The post surgery process of laying down scar tissue is carried out for about a
year. However, since radiation permanently damages DNA and normal cellular
processes, scarring typically continues for the rest of the person’s life.
The fibrin is laid down inside and outside the blood vessels,
bones, tendons, ligaments and nerves in the affected areas. The resultant
condition is called radiation fibrosis syndrome (RFS) and can occur
within several weeks or months following radiation. The intensity of the
fibrosis depends on the area, the amount and the duration of the radiation.
Other factors, such as age and medical comorbidities, also contribute to the
amount of RFS created. Rehabilitation medicine physicians with extensive
training in neuromuscular and musculoskeletal medicine, as well as in the
principles of functional restoration, are uniquely positioned to improve the
quality of life for cancer survivors with radiation fibrosis syndrome.
Many factors contribute to neck and shoulder pain after surgery
in the neck region. Education and active participation in the management
process after surgery of the head and neck are important to minimizing the
resulting discomfort. One should contact a physical and/or occupational
therapist to help gather all the tools needed to manage chronic changes.
The condition can also be treated with physical therapy and appropriate pain control. Medications such as gabapentin and carbamazepine may be prescribed. Acupuncture has been shown to decrease pain and shoulder dysfunction following neck dissection. Pain management services for treatment with narcotics and behavioral therapy are important assets in management of chronic pain.
Acupuncture can provide significant reductions in pain, dysfunction, and dry mouth in head and neck cancer patients after neck dissection.

The condition can also be treated with physical therapy and appropriate pain control. Medications such as gabapentin and carbamazepine may be prescribed. Acupuncture has been shown to decrease pain and shoulder dysfunction following neck dissection. Pain management services for treatment with narcotics and behavioral therapy are important assets in management of chronic pain.
Acupuncture can provide significant reductions in pain, dysfunction, and dry mouth in head and neck cancer patients after neck dissection.
Spinal cord stimulation may be considered
in management of chronic back, leg or arm pain in individuals that have not
found relief with other therapies. This therapy masks pain signals before they
reach the brain. A small device, is implanted in the body to deliver electrical
pulses to the spinal cord. It helps patients better manage their chronic pain symptoms
and decrease the use of opioid medications.

No comments:
Post a Comment